Special Kids & Special Needs: Understanding, Identifying, and Supporting Your Child
A baby does not respond to their name.
A toddler avoids eye contact.
A child struggles to speak while others begin forming sentences.
Parents notice these moments quietly. At first, they wait. Then they wonder.
“Is this normal?”
Sometimes, it is.
And sometimes, it is a signal that a child may need extra support.
What Are Special Needs in Children?
Special needs refer to conditions where a child requires additional support in physical, emotional, behavioral, or cognitive development.
These may include:
- Developmental delays
- Learning difficulties
- Communication challenges
- Behavioral or emotional conditions
- Physical or neurological differences
A child with special needs is not defined by limitations, but by unique developmental requirements.
Why Early Identification Matters
Early detection allows early intervention—and early intervention changes outcomes.
Research shows that timely support significantly improves developmental progress and long-term functioning (Shonkoff & Phillips, 2000).
The earlier parents recognize signs, the better the chances of improvement.
Signs of Developmental Concerns from Birth Onward
Every child develops at their own pace. However, certain delays or patterns may require attention.
Infancy (0–2 Years)
At this stage, development is rapid and foundational.
Possible Warning Signs
- Limited eye contact
- Lack of response to sounds or name
- No social smile
- Delayed motor development (sitting, crawling)
- Limited babbling or vocalization
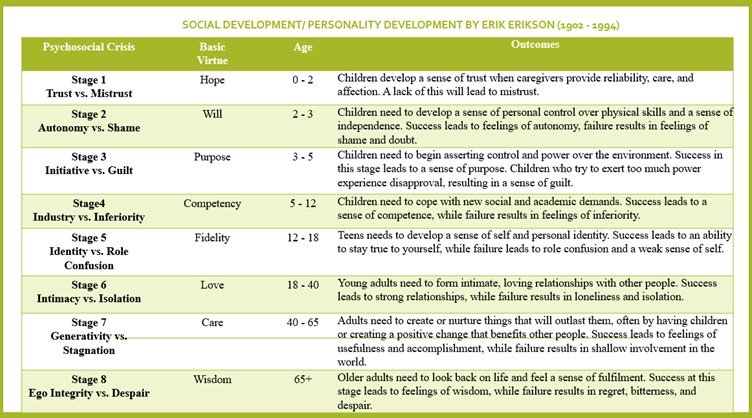
Early emotional bonding is critical. According to Erik Erikson, this stage builds trust and attachment, which are essential for later development (Erikson, 1950).
Toddler Stage (2–4 Years)
Language and behavior become more visible.
Possible Warning Signs
- Delayed speech or no meaningful words
- Lack of interest in social interaction
- Repetitive behaviors
- Difficulty following simple instructions
- Frequent intense tantrums
Early Childhood (4–7 Years)
Children begin structured learning and social interaction.
Possible Warning Signs
- Difficulty communicating clearly
- Poor attention span
- Trouble understanding basic concepts
- Lack of social interaction
- Emotional instability
Middle Childhood (7–11 Years)
Academic and social expectations increase.
Possible Warning Signs
- Learning difficulties (reading, writing, math)
- Poor memory or concentration
- Social withdrawal
- Behavioral issues
Adolescence (12–18 Years)
Emotional and psychological development becomes central.
Possible Warning Signs
- Persistent anxiety or depression
- Extreme behavioral changes
- Social isolation
- Difficulty managing responsibilities
Types of Issues in Special Needs Children
Special needs can involve different areas of development.
Physical Development Issues
These include:
- Delayed motor skills
- Coordination problems
- Physical disabilities
Children may need physiotherapy or occupational therapy for support.
Emotional Development Issues
Children may struggle with:
- Anxiety
- Fear
- Emotional regulation
- Low self-esteem
Emotional challenges often affect behavior and relationships.
Psychological and Cognitive Issues
These include:
- Learning disabilities
- Attention difficulties
- Behavioral disorders
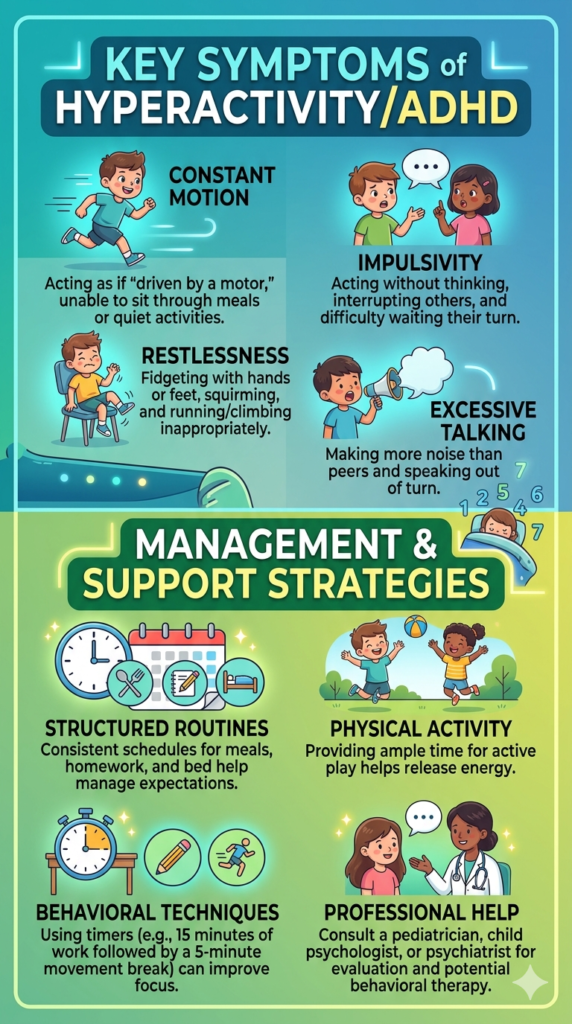
- Developmental conditions such as Autism Spectrum Disorder or ADHD
According to Jean Piaget, cognitive development progresses in stages, and delays in these stages may indicate developmental concerns (Piaget, 1952).
How to Detect Abnormalities Early
Early detection does not require medical expertise—it begins with observation.
Parents should monitor:
- Milestones (speech, movement, social interaction)
- Behavior patterns
- Emotional responses
- Learning ability
If a child consistently falls behind developmental expectations, it is important to seek evaluation.
What Parents Should Do If They Notice Concerns
The first step is not panic—it is awareness.
Consult a pediatrician or developmental specialist for proper assessment.
Early intervention programs, speech therapy, behavioral therapy, and occupational therapy can significantly improve outcomes.
According to Albert Bandura, children learn through interaction and environment, meaning supportive environments can enhance development even in challenging conditions (Bandura, 1977).
Supporting a Child with Special Needs
Support begins at home.
Create a structured and predictable environment. Children with special needs often respond better to routine.
Encourage small achievements. Progress may be slow, but every step matters.
Avoid comparison with other children. Each child has a unique developmental path.
Provide emotional support and patience.
The Role of Parents
Parents are not just caregivers—they are the strongest support system.
Acceptance is the first step. Understanding replaces fear.
Advocating for the child in school, therapy, and social settings ensures better opportunities.
Learning about the child’s condition helps in providing appropriate support.
When to Seek Professional Help
Seek immediate evaluation if:
- Developmental delays are significant
- The child loses previously learned skills
- Behavior is extreme or harmful
- Communication is severely limited
Early professional guidance improves long-term development.
Top 10 Parenting Tips for Special Needs Children
- Observe development closely
- Seek early assessment
- Follow structured routines
- Be patient and consistent
- Encourage small progress
- Avoid comparison
- Work with professionals
- Provide emotional security
- Educate yourself about the condition
- Focus on strengths, not just challenges
Final Thought
Special needs do not mean less potential. They mean different pathways. A child who learns differently is not behind—they are developing in their own way. With early support, understanding, and patience, children with special needs can grow, learn, and succeed. And the journey begins with awareness.
Read More:
REFERENCES (APA 7)
- Erikson, E. H. (1950). Childhood and society. Norton.
- Piaget, J. (1952). The origins of intelligence in children. International Universities Press.
- Bandura, A. (1977). Social learning theory. Prentice Hall.
- Shonkoff, J. P., & Phillips, D. A. (2000). From neurons to neighborhoods. National Academy Press.